About PXE
Pseudoxanthoma elasticum, (PXE), is an inherited disorder that causes some tissue in the body to become mineralized, that is, calcium and other minerals are deposited in the tissue. This can result in changes in the skin, eyes, cardiovascular system and gastrointestinal system. PXE was recognized over a hundred years ago. A number of significant advances have been made in the past few decades.
What are the signs that lead to diagnosis of PXE?
Skin
Skin changes are often the first visible sign of PXE and may help lead to a diagnosis. These changes vary from person to person and may appear at different ages.
Many people first notice small yellowish or flesh-colored bumps on the sides or back of the neck. These bumps are called papules. Over time, they may join together and make the skin look slightly pebbled, soft, loose, or wrinkled.
A dermatologist may recommend a small skin biopsy to help confirm the diagnosis. In a biopsy, a tiny piece of skin is removed and sent to a laboratory. The lab uses special stains, including von Kossa stain, to look for mineral deposits and changes in the elastic fibers of the skin.
Eyes
For some people, eye findings are the first sign of PXE. Early PXE changes in the eye usually do not affect vision and can be seen only during a dilated eye examination by an ophthalmologist.
Children with PXE may have an early retinal change called peau d’orange, a mottled “orange-peel” appearance of the retina. Some children and many adults also develop angioid streaks. Angioid streaks are small breaks in Bruch’s membrane, a thin layer behind the retina. Peau d’orange and angioid streaks do not usually cause symptoms by themselves.
Vision problems can occur if small new blood vessels grow through these breaks and leak or bleed. This is called choroidal neovascularization. It can cause distortion, blurring, or loss of central vision. Today, these bleeds can often be treated effectively with anti-VEGF injections, such as Eylea®, Lucentis®, or Avastin®.
Some people are first diagnosed with PXE after noticing distortion in their vision. If you have PXE, regular eye care is important. We recommend seeing a retina specialist and using an Amsler Grid (PDF) as instructed to check for changes in central vision. Contact your eye doctor promptly if straight lines look wavy, bent, blurred, or missing, or if you notice any sudden change in vision.
Genetics
Sometimes PXE is first suspected because of a genetic test done for another reason. A person may receive a genetic report showing two pathogenic variants in ABCC6, or one pathogenic variant and one variant of uncertain significance (VUS).
A genetic report alone does not always confirm PXE. The report should be reviewed with a geneticist or genetic counselor, especially if one of the variants is a VUS. A VUS means that there is not yet enough evidence to know whether that variant causes disease.
For an adolescent or adult with possible ABCC6-related PXE, the next step is usually to look for the physical signs of PXE. This may include:
- a skin biopsy to look for mineralization and changes in the elastic fibers in the mid-dermis; and/or
- a dilated eye exam to look for peau d’orange or angioid streaks.
If an adult has no skin findings on biopsy and no PXE-related eye findings, the person is generally not considered to have PXE based on the genetic report alone.
In infants and young children, this situation is different. Genetic testing may be done because of developmental delay, illness, or concern for another genetic condition. PXE itself does not cause severe newborn or early-childhood developmental symptoms. In a baby or young child, the child’s actual symptoms and medical findings are more important than the possibility of later-onset PXE.
There is, however, a related condition called generalized arterial calcification of infancy (GACI). GACI can sometimes be caused by two pathogenic variants in ABCC6. GACI is different from typical PXE and can cause serious mineralization of arteries in infancy. If a newborn or infant has two ABCC6 pathogenic variants and signs of illness, vascular calcification, heart problems, high blood pressure, or other serious symptoms, the child should be evaluated promptly by specialists familiar with GACI and disorders of ectopic mineralization.
How rare is PXE?
Estimates of the incidence of PXE range from 1 in 100,000 people to 1 in 25,000 people. However, the true incidence of PXE is not known in any population. It is possible that some individuals affected by PXE are not yet diagnosed (and may never be), particularly people with mild signs of PXE, or those whose signs are not typical. It is also quite likely that we do not find individuals affected by PXE in under-resourced countries and communities, and/or remote areas.
What are the effects of PXE?
PXE results in a variety of signs and symptoms. The number, type, and severity of signs of PXE are different for each person. Certain effects of PXE can cause serious medical problems while others have less impact. The effects of PXE may include: skin changes; changes in the retina of the eye that may result in significant loss of central vision; changes in the vascular system that may involve calcification of mid-sized arteries and decreased blood flow in the arms and legs; changes in the gastrointestinal system that may lead to bleeding in the stomach or intestines.
At this time, there is no way to predict the progression of PXE for a particular individual. Some people have no skin lesions; others have no vision loss. Most people do not experience gastrointestinal complications. Many experience vascular problems, particularly later in life. And a few have no signs of PXE except for a positive skin biopsy or angioid streaks in their eyes. The effects of PXE and its rate of progression seem to have no discernable pattern. Thus, there is great variability in how PXE affects each person. We see this even within families. Siblings can all have a very different experience of PXE.
What is PXE: Skin
Skin changes are often the first visible sign of PXE. They commonly appear on the sides or back of the neck and may later appear in other areas where the skin bends and flexes. The first skin changes are often small yellowish, yellow-orange, or flesh-colored bumps called papules. These may look like tiny, raised spots. Over time, the papules may group together and form larger areas of affected skin. The skin may look slightly pebbled, soft, loose, or wrinkled.
The areas most often affected include:
- Sides of the neck
- Under the arms
- Inside of the elbows
- Groin
- Behind the knees
- Navel
- inside the lower lip or other mucous membranes
Skin changes are usually symmetrical, meaning they often appear on both sides of the body.


What is PXE: Eyes
Early Eye Findings
Peau d’orange Peau d’orange means “orange peel” in French. In PXE, a mottled, orange-peel-like appearance is described in the retina. It is often one of the earliest eye signs of PXE and may appear in childhood or adolescence. It refers only to the eyes in PXE, not to skin.
Peau d’orange does not usually affect vision on its own. It is an important sign because it can help confirm a diagnosis of PXE.
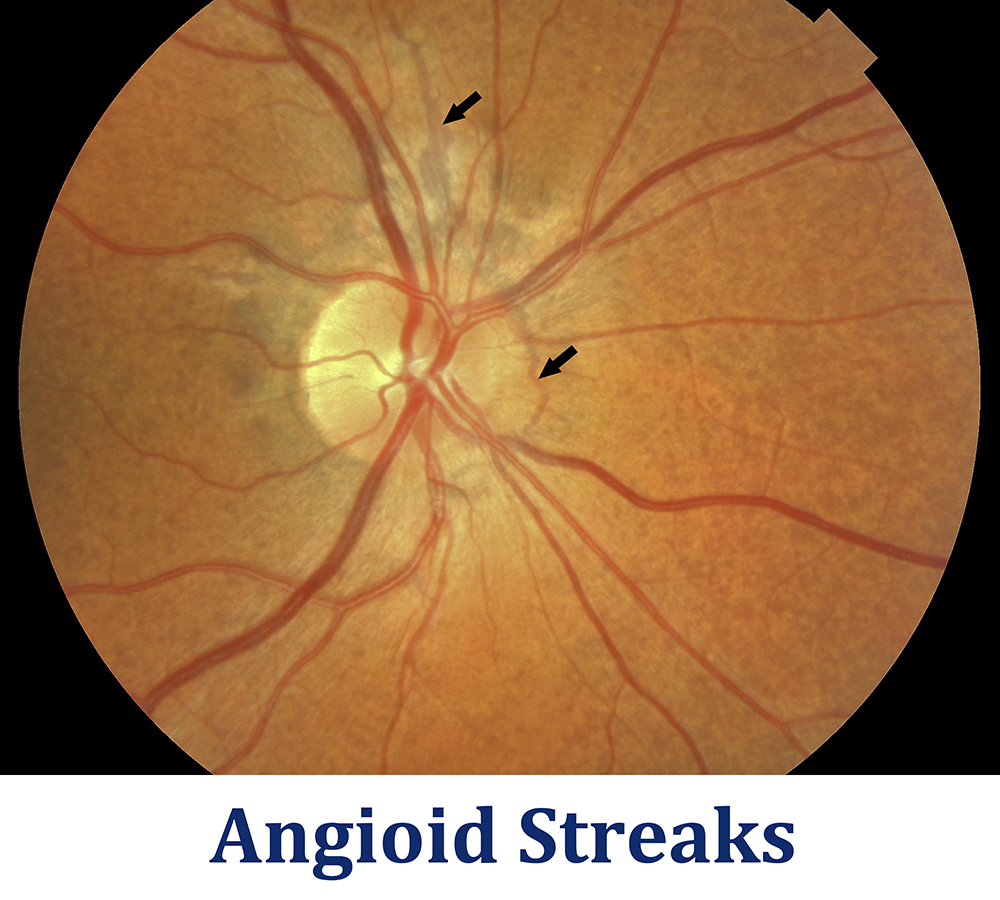
Angioid streaks Angioid streaks are small breaks in Bruch’s membrane, the thin elastic layer behind the retina. During an eye exam, they may look like reddish, brownish, or gray lines spreading out from the area around the optic nerve.
Angioid streaks are sometimes compared to fine cracks in old lacquer or dried mud. The streaks themselves usually do not affect vision, but they can create places where fragile new blood vessels may grow, leak, or bleed.
Angioid streaks do not cause vision loss on their own. However, they matter because small abnormal blood vessels can sometimes grow through these breaks. These fragile new vessels may leak or bleed.
Choroidal Neovascularization The most important PXE-related eye complication is choroidal neovascularization, often called CNV.
CNV means that small new blood vessels grow from the choroid, a blood-vessel-rich layer beneath the retina, through breaks in Bruch’s membrane. These new vessels are fragile and can leak or bleed.
When this happens near the macula, it can cause:
- Wavy or distorted lines
- Blurred central vision
- A dark or missing spot in central vision
- Difficulty reading
- Difficulty recognizing faces
- Sudden change in vision
CNV should be treated promptly. Early treatment gives the best chance of preserving vision. Check the Amsler Grid regularly for any distortion that might indicate CNV.
What is PXE: Vascular System
PXE frequently causes mineralization in the mid-laminar layer of medium-sized arteries. This causes narrowing of blood vessels, so affected individuals may have decreased blood flow to the arms and legs. Decreased flow of blood to the arms and legs may mean that one's pulse can no longer be felt in the wrists or feet. This decreased flow of blood to the arms and legs may also cause cramping or pain in the legs or arms when walking or exercising. This cramping is called intermittent claudication.
Individuals with PXE should have regular visits with their general physician to monitor blood pressure, cholesterol, and pulses in the arms and legs. A heart-healthy lifestyle is recommended, with low fat foods and plenty of exercise. Maintaining normal weight, avoiding smoking and getting consistent exercise are important ways to delay or reduce vascular complications of PXE. (Click to read more - coming soon.)
What is PXE: Gastrointestinal system
Very rarely, PXE can cause sudden bleeding in the upper gastrointestinal tract, usually from the stomach or intestines. This can be life-threatening and may not be recognized right away.
Warning signs include vomiting blood, passing black or tarry stools, unexplained anemia, faintness, weakness, or sudden dizziness. Anyone with PXE who has these symptoms should seek urgent medical care.
A person with PXE should always tell the physician that they have PXE, because gastrointestinal bleeding can be part of the condition. At the same time, the physician should evaluate the person in the usual careful way. Common causes of gastrointestinal symptoms and bleeding, such as ulcers, gastritis, medications, or other conditions, can also occur in people with PXE.
People with PXE should discuss aspirin and non-steroidal anti-inflammatory drugs, such as ibuprofen and naproxen, with their physician before using them, especially regularly or long term. These medicines can irritate the stomach and increase the risk of bleeding. However, some people need aspirin or other blood-thinning medicines because they are at risk for stroke, heart attack, blood clots, or another serious condition. In those cases, the risks and benefits should be weighed carefully with a healthcare professional. Do not stop a prescribed medicine without medical advice.
Read more: PXE Guide: Gastrointestinal Bleeding. (Coming soon)
What is PXE: Pregnancy
Most pregnancies in women with PXE are uncomplicated. In a PXE International study of 407 women with PXE, 306 women reported 795 pregnancies. Eighty-three percent resulted in live births, and gastric bleeding and retinal complications each occurred in fewer than 1% of pregnancies. The study found no basis for advising women with PXE to avoid pregnancy.
PXE alone is not a reason for cesarean delivery. People with PXE who are pregnant or planning pregnancy should tell their obstetrician about their diagnosis. Blood pressure should be monitored, and any vomiting of blood, black stools, sudden dizziness, or new vision changes should be evaluated promptly.
Read the PXE Guide: Pregnancy. (Coming soon)
Breast Calcification
Women with PXE may have benign calcifications in breast tissue, skin, or blood vessels that can appear on a mammogram. In one study, mammograms from 51 women with confirmed PXE were compared with mammograms from 109 women without PXE. Women with PXE were more likely to have skin thickening, vascular calcification, and breast microcalcifications.
Most breast calcifications seen in PXE are benign, but they can sometimes lead to extra testing if the radiologist does not know the person has PXE. PXE does not mean breast cancer is present, and PXE does not replace standard breast cancer screening. Tell the mammography center and radiologist that you have PXE so they can interpret calcifications in the right context.
Read the PXE Guide: Mammography. (Coming soon)
Testicular Calcification (Microlithiasis)
Some males with PXE have tiny calcifications in the testicles, called testicular microlithiasis. In one small study of 12 males with confirmed PXE, 11 had classic testicular microlithiasis and one had limited testicular microlithiasis on ultrasound. None had evidence of testicular cancer on ultrasound or physical examination.
These findings may be related to PXE, but the study was small. PXE should not be used to dismiss a lump, pain, swelling, asymmetry, or any other concerning testicular finding. Those symptoms should be checked in the usual way by a healthcare professional.
Read the PXE Guide: Testicular Microlithiasis. (Coming soon)
What is PXE: What kind of medical care will be needed?
Initially, a newly diagnosed individual should have assessments by a primary care physician, ophthalmologist, dermatologist, and cardiologist. People affected by PXE must find healthcare professionals who are willing to learn about PXE, since there are few well-informed professionals. PXE International has bulletins available online for many specialists including ophthalmologists, dermatologists, primary care physicians, pediatricians, obstetricians and dentists ( ).
Regular physical exams by a primary care physician are recommended. A detailed family history should be taken with regard to onset, signs that may be related to PXE and the rest of the family’s medical history. The affected individual’s blood pressure and cholesterol and triglycerides should be monitored, and abnormal levels aggressively treated. Peripheral pulses should be monitored. A dermatologist will most likely be the physician to make the definitive diagnosis and can also offer advice on reconstructive surgery if that is of interest to the patient. A cardiologist should perform a baseline EKG, cardiac stress test, echocardiogram, and Doppler evaluation of peripheral arteries. An ophthalmologist will dilate the eyes to look for peau d’orange and angioid streaks. If angioid streaks are found, it is wise to consult a retinal specialist.
What is PXE: Will other family members be affected?
PXE is inherited as an autosomal recessive disorder. This means that both copies of the gene for PXE must have a mutation for PXE in order for a person to have signs and symptoms of PXE. A person with a mutation for PXE on only one gene is called a carrier. A carrier doesn't have PXE since the working gene still performs its function. A person inherits PXE when both parents are carriers of a mutation for PXE and have both passed it on to the offspring. Each pregnancy from a union of two carriers has a 25% chance of producing a child with PXE.
Although PXE is autosomal recessive, some families have more than one generation of people with PXE. This can happen when a person with PXE, who has two PXE mutations, has a child with a carrier who has one PXE mutation (and has no signs of PXE). Each pregnancy from this union has a 50% chance of producing a child with PXE.
While there are a few families with two generations of people with PXE, there are no families with three or more generations of people with PXE. There is no autosomal dominant form of PXE, which would require only one changed copy of the gene associated with PXE to cause symptoms.
It is important to look carefully at the siblings of a newly diagnosed individual. Siblings of a person with PXE have a 25% chance of having PXE. A genetic test is available for PXE, but it does not find all mutations, and is costly. Siblings and family members of newly diagnosed individuals can have a skin biopsy to definitively diagnose PXE. They can also have their eyes examined by an ophthalmologist or retinologist for signs of PXE.
What is PXE: Where can my doctor or I get more information?
PXE International publishes informational bulletins for affected individuals and for physicians, including separate bulletins about PXE's effects on the eyes and the skin, during pregnancy, in children, and for pediatricians and dentists. PXE International publishes a newsletter in which current research projects and findings are announced and news is shared about local support groups of PXE International. These are all available by mail or online at the PXE International website. PXE International manages a registry, and blood and tissue bank, which is vital for research on PXE. In addition, PXE International initiates and funds research projects.
What is PXE: Can you recommend a doctor who knows PXE well?
We cannot recommend a doctor who is familiar with PXE, unless you are looking for an ophthalmologist or dermatologist. Contact us to ask for one of these in your area.
Since there are over 7000 rare diseases, doctors cannot be familiar with all of these diseases. Furthermore, you might find a general practitioner or cardiologist who has seen a PXE patient or two, but every person is different, and you would not want a doctor to base your care on the few other cases he or she has seen.
Fortunately, the effects of PXE on the various organ systems of the body are similar to those produced by much more common conditions – so you need to find a doctor who is caring and listens and takes the time to become educated about PXE. He or she can read our medical bulletins and learn how to care for you. He or she can also consult us (we have gathered data on more than 1000 affected individuals) if necessary.